

GENEVA SURGERY
GENEVA SURGERY
DIASTASIS RECTI
DIASTASIS RECTI
The following answers address the most common questions about diastasis recti, including its functional impact, indications for treatment, surgical reconstruction and recovery.
The following answers address the most common questions about diastasis recti, including its functional impact, indications for treatment, surgical reconstruction and recovery.
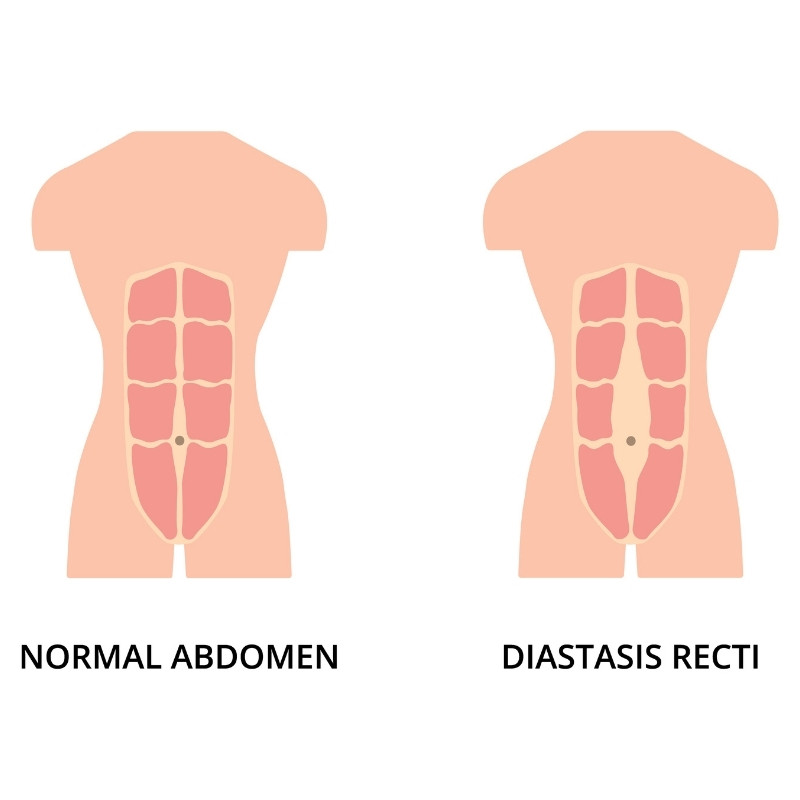
What is diastasis recti?
Diastasis recti refers to a loss of tension and continuity of the midline of the abdominal wall rather than a true hernia. Instead of efficiently transmitting forces, the abdominal wall becomes mechanically ineffective, leading to functional instability. This condition alters core mechanics and may affect posture, breathing and overall core function.
What symptoms can diastasis recti cause?
Symptoms vary widely. Some individuals notice a midline bulge, while others experience core weakness, back pain, pelvic floor dysfunction or reduced physical performance. Beyond physical symptoms, diastasis recti may affect body image and confidence, particularly after pregnancy.
Is diastasis recti only a cosmetic issue?
No. Diastasis recti is primarily a functional disorder. The objective of treatment is to restore core function and biomechanical efficiency rather than to address aesthetic concerns alone. Cosmetic considerations may coexist but are not the primary indication for treatment.
Does every diastasis recti require surgery?
Not necessarily. Conservative management plays a central role, particularly when symptoms are mild. Structured, purpose-driven physical therapy focusing on core re-education, including approaches such as Pilates and yoga, represents the cornerstone of non-surgical management. Optimisation of what can be achieved conservatively is always the first step.
When is surgical treatment considered?
Surgical reconstruction is considered when conservative measures provide improvement but remain insufficient to meet functional expectations. The decision is guided by functional impact, individual goals and shared decision-making. Completion of childbearing is not supported by scientific evidence as a strict prerequisite, and each situation is evaluated individually.
How does surgical reconstruction address diastasis recti?
Reconstruction aims to restore midline integrity and re-establish normal abdominal wall biomechanics. A minimally invasive robotic approach is used to allow precise, controlled reconstruction within anatomical planes. A specific reconstructive concept, the Inan Inverting Plication, has been developed and adopted in clinical practice to support durable reorganisation of core mechanics rather than temporary correction.
What is the role of robotic surgery in diastasis recti repair?
Reconstruction is performed using a fully robotic approach, preferentially through a suprapubic bikini-line access. This allows precise dissection in the extraperitoneal space, controlled reconstruction and accurate placement of wide extraperitoneal reinforcement. This precision supports functional restoration and predictable recovery.
How is recovery after diastasis recti repair?
Recovery is structured and individualised. Pain management follows an opioid-free strategy, early mobilisation is encouraged and functional recovery is guided progressively. The objective is an accelerated and safe return to physical activity and to the desired quality of life. Patients remain hospitalised until predefined recovery criteria are achieved, ensuring a predictable transition back to daily activities.